Part III - Healing Models and Strategies
|
|
|
|
Part III - Healing Models and Strategies
Part III of this document synthesizes the literature about healing from the standpoint of some of the major issues described in Part II: dealing with loss and grief, trauma, sexual abuse, and substance abuse. It also looks at health promotion and empowerment models which broaden the scope of the healing work from simply being free of disease, dysfunction and trauma to establishing new patterns of personal, family and community living which produce sustainable well-being. A final section briefly focuses on the need for leadership and the essential role of capacity building for person and community healing in Aboriginal communities.
A. Healing from Loss - the Grieving Cycle
Personal Loss
In Canadian Aboriginal communities it is virtually impossible to find someone who has not been touched by the loss of a loved one. Most people have experienced the death of many relatives and close friends. The tragic and often preventable nature of many of these deaths (due to high rates of substance abuse, suicide, accidents and violence) compounds the trauma associated with the loss. It is not surprising, therefore, that many Aboriginal people need help in healing from the trauma of these tragic losses, especially when another death occurs before someone has had the opportunity to grieve fully for an initial loss.
Dr. Elisabeth Kubler-Ross, through her work with terminally ill patients and their families, identified the following five stages which are commonly experienced by people confronting the inevitability of their own death and by their families and friends in coping with the loss of a loved one. These stages have come to be known as "the grieving cycle":
2. Anger - When it becomes impossible to continue to deny what has happened, the next stage is frequently anger. People ask, "Why does it have to happen to me. Its not fair." This anger can often be directed at anyone or anything around them.
3. Bargaining - In an effort to postpone dealing with a situation and feelings which seem overwhelming, people affected by the type of trauma associated with death often try to make some type of bargain with a higher power. "If I do X, then such and such will not happen." The bargain that is made often reflects guilt that people feel about something they have not done or people that they have hurt.
4. Depression - People are unable to keep up the sense of numbness associated with denial or the rage which is part of stage two. These feelings are replaced by a deep sense of loss.
5. Acceptance - If a person has had the opportunity to work through the previous four stages, he or she can come to a point of quiet acceptance of what has occurred. The acceptance stage is not simply giving up; it is moving past those feelings to a deeper understanding of the bigger patterns of life which are part of being human.
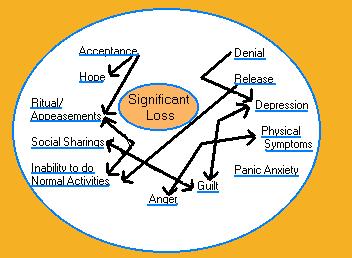
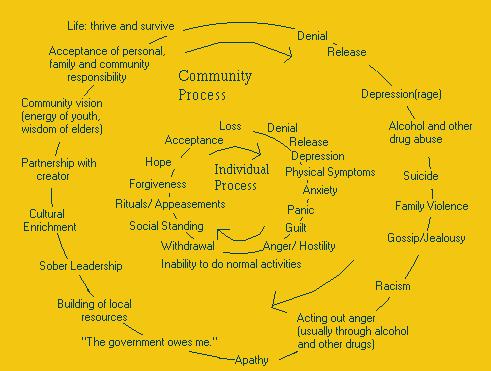
The grieving cycle model also helps us understand what happens when people are unable to complete the whole process from an initial state of denial, depression and anger to a final acceptance and the return of hope. If people "get stuck" in one stage of the grieving cycle, they continue to behave in ways which harm themselves and those around them. The results can include substance abuse, suicide, eating disorders, depression, or violence.
An important implication of this model, for the purposes of this study, is that one of the causes of personal and social dysfunction in Aboriginal communities stems from the fact that many people have been unable to work through the whole grieving process in the face of the many personal losses they have suffered. A healing strategy for Aboriginal communities must therefore include programs to assist people to move through the stages of the grieving cycle to full mental, emotional, physical and spiritual health.
Community Loss
It is not only individuals who are traumatized by loss. Whole families and communities can experience a deep sense of loss when their way of life is dramatically changed. The processes of colonization, missionization and bureaucratization to which Aboriginal people have been subjected have in many instances had the following types of consequences: poverty and the loss of self-reliance; the loss of language and cultural knowledge and traditions; the loss of strong, healthy family relationships through residential schools; the death of a significant proportion of the population through disease epidemics; the loss of control over political, social and economic decision-making processes; and the undermining of a coherent, balanced world view which gave meaning to all aspects of life.
These losses are so profound that they have had a severe impact on the capacity of some communities to create the type of social, economic, political and cultural context which nurtures individual and family health and which promotes collective prosperity and well-being. Peter Marris, in his book entitled "Loss and Change," argues that these types of collective loss actually undermine the capacity of people to learn and develop because they undermine the very structure which the culture has used to organize their relationships with each other, with the natural world and with the great unknowns. He goes on to describe the process of healing a community which has experienced a deep loss needs to go through in order to regain its capacity to work toward balance and well-being in all aspects
of life:
2. The community then needs to be able to organize its own patterns of life on its own terms without outside interference from non-members of the group.
3. Communities then can begin to restructure their world through a process of recovering their traditional knowledge and using it creatively to solve current problems and to develop a new vision of human possibility which can guide the recreation of their way of life.
B.Recovery from Trauma
During the past two decades or so, a rich literature has developed exploring the impact of personal trauma on the mental, emotional, physical and spiritual health of individuals and of collective trauma on the social, cultural, political and economic well-being of communities. Trauma can be defined as the psychological, mental and physical effects associated with a painful experience or shock. Some of the important characteristics and effects of trauma as they relate to a discussion about the healing needs of Aboriginal communities include the following:
For example, an individual can be traumatized by witnessing a brutal or tragic event (such as violent death of a parent) or by the type of persistent abuse experienced by some Aboriginal people in residential schools (by being separated from relatives, by being punished for speaking their own language and by being forced to behave in ways which are contrary to cultural norms, to eat rotten or repugnant food, or to perform sexual favours, etc.). A characteristic of chronic or repeated abuse is that it occurs in circumstances which prevent the victim from escaping. Captivity can include conditions of dependency (such as experienced by children as well as some adults), of detention (such as residential schools or prison), of poverty (which limits options) or of authoritarian power (when leadership does not allow participation in decisions which affect people).
Just like individuals, communities can experience acute trauma (for example, when a disease epidemic wipes out a significant number of their population or a disaster destroys their property and livelihood) or chronic abuse (such as through a process of colonization which repeatedly attacks the foundations of their culture and social organization).
2. Trauma, regardless of the form in which it was experienced, has certain characteristic effects on individuals and the way in which they perceive the world around them.
All forms of psychological trauma have in common their capacity to engender feelings of "intense fear, helplessness, loss of control, and threat of annihilation" (Andreasen 1985:918). Erikson (1994:21) describes the symptoms of trauma as "a numbness of spirit, a susceptibility to anxiety, rage and depression, a sense of helplessness, an inability to concentrate, a loss of various motor skills, a heightened apprehension about the physical and social environment, a preoccupation with death, a retreat into dependency, and a general loss of ego functions.
Trauma not only affects an individuals psychological health, but also the capacity of that individual to connect with others in healthy relationships and to bond with community institutions and social structures. Trauma affects whole communities by undermining social, cultural, economic and political structures and relationships as well as the capacity of that community to interact in a healthy, balanced way with the society around it. Trauma can also undermine spiritual beliefs. People lose faith not only in human institutions but in the divine law and justice.
When trauma is prolonged or repeated, it can result in a sense of helplessness and hopelessness, both on an individual and a collective (family or community level). People lose faith in their capacity to control their own lives. Fear and a sense of helplessness can seriously affect the capacity to learn, and in this way the impact of trauma can make it difficult for an individual or community to heal from the shock, to return to some sort of balance and harmony, and to behave in the future in ways that
will minimize the likelihood that the trauma will be repeated.
In summary, trauma affects the sense of self, the relationships people have with each other and their entire world view. Healing efforts aimed at helping individuals and communities overcome the affects of trauma must therefore work on all three of these levels.
3. Chronic childhood trauma results in a particular set of behaviours and adaptations known in the psychological literature as codependency.
Chronic childhood abuse can be physical (e.g. neglect, battering), sexual (e.g. incest, rape, fondling), emotional (e.g. verbal abuse, neglect and abandonment), intellectual (e.g. when children are not allowed to do their own thinking), or spiritual (e.g. when a childs spiritual beliefs and practices are ridiculed or forbidden by residential school staff or when the abuser is a representative of a religious organization). Prolonged childhood abuse is especially harmful when it gives the child the message that he or she is helpless and that the abuser is all powerful.
Codependency is a term that has become a popular way of describing the type of behaviour which individuals adopt in order to cope with chronic childhood abuse. It is also a set of behaviours which are learned in families and communities which have not healed themselves from past traumas. Codependency has been defined by Wegscheider-Cruse and Cruse as "a pattern of painful dependency on compulsive behaviours and on approval from others in an attempt to find safety, self-worth and identity." Pia Mellody identifies five symptoms which form "the core of the disease":
An approach to family counselling which has been called family systems theory, argues that a certain way of thinking and behaving (e.g. codependency as described above) can become institutionalized in a particular family or community culture. In this way, a particular way of responding to an initial trauma becomes accepted as a "normal" way of life. Because those behaviours and ways of thinking are not balanced and healthy, however, they continue to inflict fresh trauma on everyone who has part of the family or community and thus are perpetuated from one generation to the next.
Some of the types of behaviour which can become part of a dysfunctional generational pattern of life include: strong feelings of helplessness, dependence and inferiority; high incidences of alcoholism, other drug abuse, sexual abuse, domestic violence and suicide frequently resorting to violence to settle quarrels; early sexual initiation and high incidences of sexual promiscuity; a high proportion of single-parent families headed by women; little ability to defer gratification and plan for the future; low levels of cooperation to work toward the common good; a mistrust of societal institutions and authority structures; and a sense of resignation and fatalism.
While some of these behaviours may appear to be logical or reasonable for communities which have suffered chronic abuse, the problem is that these same behaviours inflict fresh trauma on community members and make it very difficult for the community to recreate its institutions and relationships in ways which lead to well-being and prosperity. For example, it is entirely reasonable for communities which have been colonized to mistrust societal institutions and authority structures. On the other hand, unless the people in those same communities are overcome their suspicion and mistrust in order to build local institutions and power relationships which are healthy and which work for the common good, the existing pattern of life becomes abusive in itself. This can be called a type of "internalized oppression" in which the victims create relationships through which they continue to abuse each other.
5. Not just individuals but also social collectives can sustain traumatic wounds.
Communities can be traumatized by natural disasters such as earthquakes, floods or epidemics or through the actions of human beings such as wars, environmental degradation, the forced dislocation of people from their homes, the destruction of a communitys economic base, chronic poverty and dependency, the devaluing or outlawing of a peoples cultural and spiritual practices, the loss of language and traditional knowledge, the loss of young people to substance abuse and suicide, or the loss of strong family relationships through residential schools.
When whole communities are traumatized in these ways, a significant proportion of the population will feel powerless and disconnected rather than creative, responsible and united. Social institutions will tend to reinforce dependency, learned helplessness, corruption and mistrust rather than productivity, an orientation to service and "common-unity." People will not feel bound together in a supportive network of relationships which can sustain them through hard times and create a sense of purpose and meaning for life.
Some Aboriginal people have referred to the
conditions in their families and communities as reflecting the "residential
school syndrome"--the incorporation of the behaviours learned in struggling
to cope with the chronic abuse of residential schools into everyday life,
even long after the residential schools have been closed. Duran and Duran
(1995:30-34) have described this phenomenon as inter-generational post
traumatic stress disorder.
The process of recovering from trauma requires a number of conditions or features in order to be successful.
The family or the community can also create conditions which make it safe for individuals to do healing work. Strong interpersonal bonds which are non-judgmental and supportive and which foster autonomy rather than dependence are essential. As well, collective solidarity in a community through a shared sense of history, language, values, traditions and ceremonies and identity are important. Community leadership which acknowledges the importance of healing, which creates space and legitimacy for healing processes and which is willing to undertake their own healing journeys can also be a powerful catalyst for healing.
Of course, the dilemma here is that people who are traumatized have a very difficult time creating family and community cultures which are safe for healing work. Their own trauma prevents them from forming the type of interpersonal relationships and community institutions which will support healing. As well, their own trauma can continually be re-stimulated through the behaviour of individuals who are not yet ready to begin healing work or who are beginning the healing process through grieving for what they have suffered and lost. In this case, resources from outside of the community will be needed to help create a safe place for the healing work to begin and to build up the trust and networks of mutual support which will allow it to continue.
2. Discharging - People need to acknowledge the harm they have experienced and discharge their feelings of grief, anger and despair. People who have experienced profound loss need to tell their stories, often many times. If properly handled, this stage allows people to move past denial and through depression and anger to a readiness to begin moving toward a new understanding of their potential and purpose as human beings.
This stage is a challenging one, because breaking through the numbness of denial or depression in order to face what has occurred can seem overwhelming and be very painful. The telling of the story brings with it all the feelings of violation, fear, powerlessness, rage and shame which are part of being a victim of abuse or other types of trauma. It is also challenging because many people will resist completely facing their pain by focussing on seeking revenge or compensation or on simply forgiving the abuser. To say this does not mean that compensation is not often appropriate or that coming to the point of being able to forgive your abuser is not admirable. Trauma therapists, however, note that these steps cannot really be taken effectively if the victim is doing them in order to avoid working through the process of remembering the pain which has been suffered and grieving for what has been lost.
3. Reconnection - Since feelings of helplessness, isolation and a lack of trust are the primary long-term harmful effects of trauma, an essential next step is for the victim to reconnect with themselves and with others in fulfilling and constructive ways. This means first of all that the individuals who are going through a healing process have to re-examine their basic beliefs about themselves, or, as it is sometimes described, to create a "post-trauma self". Trauma has such a profound effect on people that it often shakes their view of themselves, of their self-worth, of their purpose for living and of their capacity to be loving, creative, intelligent beings. Creating a new self can involve re-learning what it means to be an ordinary, healthy human being because the victims sense of such things as appropriate intimacy boundaries as well as appropriate emotional expressions can be distorted as a result of the trauma. It involves changing both beliefs and values as well as behaviour. It also usually means moving past a definition of oneself as a victim, forever powerless and fearful. It means accepting responsibility for the future and taking important first steps to become constructive members of society and to develop ones mental, emotional, physical and spiritual potential.
As this new self is being born, the individual healing from trauma must begin developing trusting, caring relationships with others. This process often begins through a deep relationship with a healer of some sort, whether trained through western medicine or through traditional processes. This is one reason why healers must behave in completely honourable ways which will enhance the capacity of the traumatized person to build appropriate relationships built on the new, "post-traumatic self". The relationship of trust, mutual respect and confidentiality which begins with the healer can then be extended in appropriate ways (i.e. while honouring appropriate boundaries) to others in society. It is through these relationships that people can express and exercise such capacities as autonomy, courage, intimacy, and initiative. It is at this point that the victim is ready to work toward seeking justice or compensation for the harm or loss incurred and toward forgiveness for the abuser, not because the act that was committed is excusable, but because of a deep appreciation for our common humanity.
Some of the capacities and skills which need to be built include decision making, coping effectively with stress, effective communication and human relations, life skills concerning meeting basic needs and setting goals and priorities for life, exercising positive values and ethics, working with others on issues of common concern, having satisfying work and fulfilling career aspirations, and maintaining positive mental and physical health.
5. Building a New Pattern of Life - A final stage of the healing journey is building a pattern of life which ensures that the basic conditions of health and well-being are met. These conditions are sometimes called the determinants of health, and include such things as being able to meet basic physical needs; having a strong cultural and personal identity; feeling safe and secure; having mutually supportive relationships with family, friends and neighbours; having access to appropriate human services; being engaged in meaningful work and service to others; having a strong connection with life-sustaining values, morals and ethics; having opportunities to learn and develop throughout the life span; and having a voice in the decisions which affect your life.
Obviously, the individual can not create all these conditions for sustainable well-being alone. While individuals can make many decisions concerning life-style and life choices, this work also requires concerted effort by families, community organizations, the community as a whole, and government at the local, regional, provincial and national levels. A section below on community healing fills in part of this picture. The parts of this chapter concerning health promotion and empowerment models also discuss strategies for tackling this component of the healing process.
In most Aboriginal communities, it is not only individuals which have been traumatized, but whole families and communities. This concept has already been mentioned in the section above on "Community Loss." The loss of language and culture, the loss of self-reliance and an economic base, the loss of whole families and communities through disease, the loss of whole generations of children to residential schools, and generational patterns of alcoholism and sexual abuse are all examples of the types of prolonged trauma suffered by many communities.
Since it is the supportive networks which are part of a healthy community which help make it possible for individuals to heal from their own abuse, these collective traumas are doubly harmful. First, traumatized communities create an environment in which it is difficult for individuals to do their own healing work. The community traditions, cultural processes, and institutions which formerly would have allowed traumatized people to tell their stories and process their emotions have broken down. Relationships5493h family, friends, neighbours and community workers or leaders no longer provide a safe haven for rebuilding the capacity for trust and intimacy. Reconnecting with a community which is not functioning in life-enhancing ways will not necessarily be a step toward recovery.
Secondly, these communities themselves must also go through a form of collective healing in order to be restored to balance. This process can be a long and painful one and it requires the same types of conditions as are required for individual healing, but on a much larger and more prolonged scale in order to be successful.
The effects of collective trauma are very pervasive. They tend to destroy the
foundation of trust and the capacity to work together for the common good which are a prerequisite for healthy formal and informal institutions and patterns of economic, political and social relationships. Many individuals in the community will have lost faith in authority and many leaders, themselves traumatized, may no longer be worthy of trust. In other words, the network of social relationships and institutions which would ordinarily make it possible for a community to begin to do its healing work has been destroyed and has to be recreated at the same time as the individuals in the community have to become healthy enough to create an environment in which others can heal.
Like individuals, communities must establish a type of therapeutic relationship with helpers or resource people who can create a safe, holding environment in which they can focus on healing work. These helpers must model beneficial values and behaviour in order to help the community establish a "post-traumatic identity"--a new vision of human potential based on sound ethical principles, grounded in cultural knowledge and capable of solving critical social and economic issues.
These helpers can also help guide the community through processes designed to tell their story and to grieve their losses. And they must help the community recreate bonds of trust, mutual aid and creative self-reliance. These helpers can be traditional healers, spiritual leaders, community development workers, other formal and informal community leaders. If these helpers come from within the community, they often need the support of outside helpers to be able to perform this difficult function in the face of opposition, scapegoating, and feelings of hopelessness and despair.
Community Healing Steps and Conditions
The steps which a community must go through in order to heal--to move out of a vicious cycle of violence, blaming, despair and self-destructive behaviour--can be summarized as follows:
2. This process requires leadership. In most instances, this leadership comes from two sources:
b. outside helpers who provide support to the inside leadership and who are able to bring badly needed resources such as learning processes, connection with other communities which have successfully dealt with the same issues, and a neutral outside perspective which can be trusted by community members.
4. Bonds of trust and mutual aid must be re-established within families and between community members. This can be one of the outcomes of people sharing and processing feelings together through the types of experiences listed in #3 above. It can also be a conscious step which people take as they come together to tackle some of the critical challenges they face, such as reducing youth substance abuse or preventing youth suicides. At some point community members must realize that they will be unable to move forward without learning to trust each other and to create a foundation of unity. Building these new relationships will not just happen. It will require dedicated effort to overcome the old patterns. It will also require facing up to and moving past old hurts and grievances.
5. In all likelihood, dysfunctional communities will have dysfunctional community organizations and agencies (whether professional or volunteer). The formal and informal institutions in the community need to be transformed in accordance with life-preserving, life-enhancing principles and processes. In other words, organizational healing processes following the steps outlined in this section will also be needed.
6. A new pattern of individual, family and community life must be built. This step requires a process of community consultation, often over a period of many months or even years, in order to articulate a common vision for the future and the core principles which must guide the development process (based on a deep understanding of cultural values and identity). In other words, the community must come together to answer such questions as:
6. Through all of the above steps, the community must keep learning. Individuals, families and communities who are traumatized often have a reduced capacity to learn. Their struggle to control strong feelings of anger, fear, helpless or hopelessness has not left them much energy for creativity and learning. As well, personal and cultural identity and perceptions about self-worth have become distorted. Through the healing process, these feelings are released and the individual and community is ready to adopt a new, "post-trauma" identity (see the section on healing from personal trauma above). This will require new information, skills and attitudes related to many issues: personal well-being, interpersonal relations, leadership, and dealing with critical social and economic development issues. The need for capacity building as part of the healing process is dealt with in more detail in a later section of this chapter.
7. The community must establish healthy relationships with other communities around it on the basis of its "post-trauma" identity. These renewed relationships are a necessary part of establishing viable economic, social, political and cultural patterns in the context of regional, provincial, national and international forces.
2. Guilt - Children often feel that the abuse was somehow their fault. They may also feel guilty about the consequences which the abuser is facing or for feelings of anger toward other adults who have not protected them. Another source of guilt can be the pleasurable feelings which sometimes accompany abuse.
3. Fear - Child victims may be afraid of many things, for example, of the abuse happening again; of being helpless to protect themselves; of retaliation by the abuser for telling; of rejection by the abuser, the spouse of the abuser and other family members; of not being believed; of "causing trouble" by telling; of being labeled (stigmatization) as having a bad reputation, or being low or dirty; of being pregnant, or about sexual myths they have come to believe concerning what would happen to them; of being alone with an adult (male or female); of bathrooms or showers; of going to bed or to sleep
4. Low self-esteem - Most victims develop very bad opinions of themselves. They can feel no good, dirty, damaged, powerless, stupid--like nothing good could ever come from them. If you feel bad about yourself, it is hard to love or trust anyone else. Low social skills often are a part of poor self-esteem. The child doesn't know how to make or keep friends, end failed relationships, making self-esteem even lower.
5. Depression - Signs of depression include feeling sad, withdrawn, subdued, tired much of the time, or chronic sickness (colds, flu, etc.). Extreme depression can lead to suicidal feelings and attempted suicide.
6. Anger and repressed hostility - Although on the outside, many child victims appear to be passive, most of them are inwardly seething with anger and hostility. They are angry at the abusers, parents and other family members for either failing to protect them, or even for somehow cooperating to allow the abuse to happen (looking the other way, etc.). Because they have been victims of a violation involving power, they have had to stuff the anger inside of them so it doesn't show. If not brought out, this anger can eventually cause physical sickness, rage, serious depression, violence or suicide in later life.
7. Impaired ability to trust - Victims of sexual abuse have been violated, usually by someone in a position of trust (e.g. a parent, a sibling, a close relative, or a family friend). This betrayal makes it very hard for some children to believe it is safe to trust anyone. Often promises made to the victim were broken. Sometimes the entire family turns against the victim, showering her with hatred and rejection for "telling lies" about Dad (or whoever). In such a case, all the people in whom the victim has trusted have (in the victim's eyes) broken that trust. The victim is alone and learns that to trust anyone is painful and dangerous.
8. Difficulty distinguishing between affection and sexual behaviour - Children who have been sexually abused are often "old for their years" in sexual matters. They know too much. They often respond sexually (i.e. seductively) at young ages. Confusing sex with affection is common, especially between female victims and men in general. These victims need to learn that men can be affectionate without sex.
9. Blurred boundaries and roles - Healthy families and societies have clear boundaries and roles that describe appropriate and inappropriate sexual behaviour . These roles and boundary rules also describe the important differences between an adult and a child. Sexual abuse of children violates these normal roles and boundaries needed to keep people healthy. When this blurring of roles and boundaries occurs, the child victim becomes confused and becomes unable to tell what is or is not appropriate.
10. Pseudo-maturity and uncompleted developmental tasks - Victims of abuse (especially if it goes on over a long time) often become preoccupied with sexuality and the abuse relationship. In father-daughter incest, the victim may end up taking over many of the roles of the spouse (housekeeping, parenting other siblings, and general family caretaking, on top of the role of sexual partner). This sometimes happens in alcoholic families as well, even if no sexual abuse is occurring. The consequence for the victim is they don't go through the normal processes of growing up, such as having close friends. "She is eleven going on thirty," describes such children.
The healing goals and steps for children who are victims of sexual abuse include:
2. Being believed regarding the reality of the abuse;
3. Acknowledging feelings connected to the abuse, and venting negative emotions;
4. Knowing the abuse was "not my fault," and that adult abusers are responsible for their actions;
5. Knowing that the adult world considers the abuse wrong and a violation of proper boundaries;
6. Knowing that she/he is not "damaged goods" and is okay physically and in every other way;
7. Learning age-appropriate expressions of affection and learning to be assertive and to say "no" to inappropriate expressions;
8. Strengthening the child's self image and self-esteem;
9. Strengthening the child's sense of self mastery and agency (empowerment; volitional
development);
10. Receiving adult support in dealing with anger and hurt;
11. Learning how to communicate needs and feelings with words; and
12. Learning positive means of coping with the abuse to replace negative patterns the child is using.
Adult survivors who have not yet gone through healing processes have all the same feelings and issues as child victims, because most survivors were child victims. As children, survivors learned in the best way they could how to cope with life, but many entered adulthood with handicaps and scars.
Most adult survivors still carry guilt, fear, low self-esteem, a feeling they are damaged goods, depression, rage and repressed hostility, great difficulty in trusting others, problems in their own attempts to find affection and healthy sexuality, a difficulty with boundaries and roles (which can lead to becoming an abuser), uncompleted developmental tasks, and a general sense of powerlessness.
On top of all this, adult survivors have to deal with the consequences of their own dysfunctional thinking, feeling and behaviour . In other words, there are two layers (at least) of issues. The first relates to the stored up feelings from childhood abuse. The second relates to un-learning and re-learning how to be a balanced, healthy, happy human being.
Sometimes victims respond to abuse with more extreme psychological responses. Usually this happens when victims have been severely traumatized, when abuse lasts a long time, when the aftermath of disclosure is particularly painful, when a victim has been victimized by more than one abuser, and to victims of "ritualistic or bizarre abuse."
the body" and travel with mind and emotions to the safe place.
2. Multiple Personality Disorder (MPD) - This is a condition in which two or more (sometimes dozens or more) "people" or personalities exist within the same individual. One personality may be invincible from hurt, another angry and raging about the abuse, another in complete denial that the abuse happened, and yet another is the victim. Changes from one personality to another can occur suddenly. Some studies have shown that many cases of MPD are incest victims. By being someone else other than the victim, the victim can avoid having to directly confront the trauma of the abuse.
3. Post Traumatic Stress Disorder (PTSD) - PTSD can occur when a person experiences a very distressing event that is outside the range of anything ever experienced before. The event would most likely be distressing to almost anyone. Events like witnessing a brutal murder, seeing a loved one killed in an accident, a serious threat to one's life or to one's family members, etc. Children living in war zones often suffer from PTSD. Some of the symptoms include flashbacks and dreams causing the continual re-experiencing of the traumatic events; intense emotional pain at being exposed to the news of similar events (including anniversaries of the trauma); avoidance of anything to do with the trauma (talking about it, etc.); constantly being nervous, on edge, uptight, leading to unpredictable outbursts of anger or weeping, difficulty sleeping, and an inability to concentrate.
The adult survivors healing journey must deal with most of the same issues as described above for child victims, but it usually takes a somewhat different course. Suzanne Sgroi outlines the following stages of adult survivor recovery:
One of the first steps an adult survivor can take toward healing is to break through the self-protective denial to see how the abuse that happened as a child (and the memories of the abuse) helped to shape the dysfunctional patterns in the survivor's life today. Remembering also means allowing oneself to remember the feelings connected to the abuse and to acknowledge they are real.
2. Recognizing survivor responses to the abuse - The next stage is learning to recognize the dysfunctional patterns of today's life as survival responses. Two levels of survival response occur:
Unless a community has a mechanism for doing this safely, such as a response team which is empowered by law and agreement; and is trained to do such intervention, confronting the abuser should be left to professionals who have legal and program responsibility to do the job. If confronting the abuser is not handled properly, the result could be denial and permanent cover up of the abuse, further abuse (or worse) for the victim, as well as violence or the suicide of the abuser, the victim, the spouse of the abuser or even someone in the community who is reminded of their own unresolved abuse. Suffice to say here that confronting the abuser is part of the healing process, and that it takes preparation, prior agreements, and in-depth training to do it effectively.
Sgroi describes recovery as an ascending spiral of a) acknowledging reality of the abuse; b) overcoming secondary responses to abuse; c) forgiving one's self; d) relinquishing survival identity and moving beyond. This cycle then repeats, over and over again--acknowledging reality, overcoming secondary abuse, etc.
Substance abuse does not happen for one simple reason, or even for several specific reasons. Rather, substance abuse is part of a much larger pattern of life which includes many factors. It is a clear indication that something is out of balance in the lives of individuals, families and communities. There are many factors in the lives of individuals and in the social-cultural environment in which they live that have been associated with substance abuse. These are commonly called risk factors because when these factors are present, people are at a higher risk of suffering from substance abuse as well. Three general risk factors which have been associated with substance abuse in Aboriginal communities can be summarized as follows:
Because substance abuse is closely related to other types of social problems, one of the related ideas that is stressed again and again in the literature is that recovery involves a great deal more than merely stopping the abuse of certain substances. Unless the whole pattern of life of which substance abuse is a part is transformed through some sort of healing and development process, the problem behaviours will simply re-appear in another form, usually through other types of addictive behaviour such as gambling, over eating, workaholism, sexual addictions or dependence on the welfare system. Sometimes this larger pattern of life which is closely associated with addictions of all types is called "co-dependence." Some of the common characteristics of co-dependence include:
- confusion is the norm and an excuse for not taking responsibility for our lives.
- denial is the addict's major defense. We do not have that problem. Denial allows us to avoid coming to terms about what is really going on.
- forgetfulness - ranges from misplacing car keys to blackouts.
- perfectionism - nothing you do, or anyone else does, is quite good enough; mistakes are unacceptable. If we do make a mistake, we have to cover up and deny.
- dependency - assuming someone or something outside yourself will take care of you and that you cannot take care of yourself. We became "dependent" on relationships, processes (like work or sex), substances (like alcohol or food), and systems (like welfare)
- scarcity model thinking - never enough to go around so get all you can right now.
- negative thinking - perceiving self, others, situations as negative. Rather than seeing possibilities, we see only limitations.
- defensiveness - we cannot respond to feedback or criticism. Instead we must prove we are right. No real learning or change occurs.
As well, when substance abuse has been used as a strategy to numb the pain associated with the deep personal loss, sexual abuse or other types of trauma, then the healing process must encompass all of these other issues. Unless it does so, the individual may simply become overwhelmed by feelings of fear, anger, despair, and pain and may revert to the substance abuse or even commit suicide.
Another important point to consider is that an addict is usually part of a whole system of inter-personal relationships which supports his or her behaviour and allows the family and close friends to cope in a very difficult situation. For this reason, it is not only the addict who needs healing, but this web of family and friends who need to learn new, healthier ways of thinking and acting. Some of the common roles played by those close to an addict include the following:
High rates of substance abuse have many harmful consequences for communities. Some of the problems include the following. Economic productivity suffers because individuals are unable to work consistently and effectively. Children, young people, elders and other dependents are neglected and abused. Crime rates rise. Social services, education and health services are strained due to the added pressures for their services. Death, accident and illness rates also go up. Family violence, sexual abuse and family breakdowns also undermine the stability of the community.
Just as important as all of these economic and social problems which accompany high rates of substance abuse, is the breakdown in the relationships which make it possible for the individuals, families and organization in the community to work together for a common purpose. Just as your body gives you warning signs when you are getting sick, so too there are clear signs when a community and the organizations in it are losing balance and direction. And if it does, it cannot bring about health for the people. At best it will be ineffective; at worst it will make people sicker. What follows is a list of warning signs that a community needs a healing process to recover its capacity to promote health and well-being for its people.
2. Backbiting
3. Disunity
4. No time for vision (too busy dealing with crises)
5. All talk; no action
6. Personal dysfunction prevents people from contributing to community goals and well-being
7. People are continually undermining decision-making processes
8. No reality checks
9. There is no room for people to express and deal with their feelings
10. Personal conflicts affecting the way group work together to achieve community goals
11. Different parts of the community (e.g. the administration and the social service programs) are not working together for the same goals
12. Not walking the talk
13. No space for spirituality or on-going conflicts about spiritual matters
14. Individuals, families, and community organizations are not continually learning new skills and gaining new information
Healing from Substance Abuse
What follows is a brief summary of the steps which are commonly described as part of the healing journey for both addicts and those family members and friends who have developed co-dependent patterns of dealing with the abuse. These steps do not necessarily have to occur in the sequence presented, but rather they often overlap each other.
Because substance abuse is part of a much larger dysfunctional pattern of individual, family and community life, it is not only individuals who must go through a healing journey. Families, community organizations and the community as a whole must also move past the ways of thinking and acting which have helped to give rise to the problem in the first place. Following are some of the steps which have been identified as essential for recovery from substance abuse on the community and organizational level.
All of the healing models associated with the specific issues discussed in this chapter are clear that dealing with trauma, grief and addiction is only one of the steps in the healing process. Equally important is developing the capacity of the individual, of families, of community organizations, and of the community as a whole to move past illness and to reach their full potential. A clear implication of this realization is that intervention and treatment programs related to specific healing issues need to be linked with comprehensive community health promotion initiatives.
The field of health promotion achieved a major milestone in 1986 when a World Health Organization conference held in Ottawa, Canada released a document entitled the "Ottawa Charter for Health Promotion, which synthesized and built on much of the thinking to date. This model still serves as a reference point for the development of many health promotion initiatives and so it is worth presenting in a summary fashion.
The definition of health promotion presented in the "Ottawa Charter for Health Promotion" is:
2. Create supportive environments - There are many kinds of environments which need to be protected in order to create healthy individuals, families, organizations and communities. These include the physical environment (e.g. the quality of the air, water and soil), the social environment (e.g. the quality of human relationships in families and the community and the degree to which diversity is valued), and the environment in the workplace (both physical and social as well as the degree to which workers feel a sense of control and satisfaction in their role). This line of action also has to do with the degree to which community members share in the important decisions which affect their lives.
3. Strengthen community action - This line of action concerns the capacity of groups within the community to address specific determinants of health by setting priorities, making decisions, identifying and implementing effective strategies and monitoring and evaluating the results of their activities. At the heart of this process is the empowerment of communities to take responsibility for those preconditions of health which can only be addressed through their full participation and collective action. According to the Ottawa Charter, effective community action requires "full and continuous access to information, learning opportunities for health, as well as funding support." It also means developing mechanisms for meaningful and on-going input into public health policy and local, regional, provincial and national programme development.
4. Develop personal skills - Required skills are those which directly relate to preventing and coping with disease or injury and making personal life-style choices which enhance personal health (e.g. with respect to nutrition, fitness, the use of substances such as tobacco, alcohol and other drugs). Equally essential are skills which assist people to address determinants of health such as creating social support systems, finding meaning and purpose in life, participating in meaningful work and service to the community, and working with neighbours and community agencies to ensure peace and security for all members of the community.
5. Reorient health services - In order to achieve optimum well-being, people need not only to be free from disease but to have the capacity and resources "to identify and to realize aspirations, to satisfy needs, and to change or cope with the environment" (Ottawa Charter). This means that health services will have to shift their focus from a primary orientation to providing "sick care services" to one which balances this vital need with health promotion initiatives designed to address the determinants of health. This step will require new and creative partnerships both between health services and local communities as well as among community institutions and services of all kinds (e.g. strong collaboration between health, social service, economic development and education programs). In order to do this, health professional will need to reorient their attitudes and approaches through new types of training.
As health promotion practitioners struggle to implement models such as the one presented above, it has become clear that a great deal of work still needs to be done in order to integrate this way of thinking into general public policy and mount initiatives which clearly demonstrate the efficacy of this approach. One step in this direction has been the further clarification of the dimensions of a comprehensive health promotion model. The chart at the top of the next page illustrates an approach which has proven to be useful in the efforts of Canadian provincial health authorities to strengthen their health promotion programs.
Capacity Building Domains
This model also identifies the following domains in which communities need to build capacity in order to do effective health promotion work:
Actions at various levels:
Society Institutions Community Family Individual
HOW
Strategies:
Build healthy public policy Create supportive environments Strengthen community action
Develop personal skills Reorient health services Reduce inequities
WHAT
Determinants:
Basic phys-ical needs Spirituality and a sense of purpose
Life-sus-taining values, morals and ethics Safety and security
Adequate income and sus-tainable economics Adequate power
Social justice and equity Cultural integrity and identity
Community solidarity and social support Critical learning opportunities
Strong families and healthy child development Meaning-ful work and ser-vice to others
Adequate human services and social safety net
Health eco-sys-tem and a sustain-able rela-tionship between human be-ings and the natural world
A final component of the model is an articulation of the principles which need to be honoured in order to ensure that health promotion work will lead toward long-term well-being and prosperity. These principles are essentially the same as those presented in Part I of this document and so they have not been replicated here.
Supporting Community-based Health Promotion Activity
A basic health promotion model needs to be adapted and fleshed out for each particular locality or context. In general terms, agencies and front-line workers who are trying to stimulate community health promotion initiatives can use a process which includes the following steps to ensure that this happens:
The field of health promotion provides a very important addition to the literature on healing models related to loss and grief, trauma, sexual abuse and addictions. It focuses attention on the work that must be done to move individuals, families and communities past disease, addictions and trauma to a fuller realization of their potential in all aspects of life and a fuller participation in initiatives designed to address all the determinants of health. Health promotion models provide a description of all the dimensions which must be taken into account in order achieve this:
The term "community" literally means common oneness. Imagine a small family living alone in the wilderness. Everything that family needs in order to survive must be obtained through their own knowledge, skills and labour. If they need food, they must either hunt it, gather it, or grow it. Clothing must be made from skins that are tanned or cloth that is made of fibers which must be gathered, treated or spun, sometimes dyed, and finally woven. This goes for everything from shelter, tools and traveling technologies to medicines and artistic or religious expression.
Now imagine that several families meet and begin to compare their lives. They quickly realize that if they banded together, some things would be much better and easier for everyone. The women could help each other with gathering food and fuel and with child rearing. The men could much more easily ensure the protection of their families from predators and enemies and could also collaborate for certain kinds of fish and game harvesting. Everyone would benefit in such arrangements from the social life that would be created simply by having more people together.
However, there were also drawbacks. In order to get along, people had to make roles and establish boundaries (such as, taboos against talking to your mother-in-law or wife's sister, probably to avoid family conflict or sexual tensions.). As more and more people grouped together (depending mostly on the economic carrying capacity of the land and the people's capacity to produce food), life became more and more complicated. People negotiated their relationships with each other to maximize the collective good, adding hierarchies of power, protocols for getting things done without upsetting the social order, and codes of conduct to protect the well-being of everyone.
The entire process described here is really community development--the development of the web of relationships within which people live for the purpose of maximizing the common good.
We have seen in Part II how the advent of Europeans to the North American continent set into motion a number of social, cultural, political, economical and even biological forces that had a tremendous impact on the way of life of Aboriginal people. Missionization, trade and colonization, bureaucratization, European schooling and disease all took their toll on the many communities and nations of Aboriginal people scattered across the continent.
There can be little doubt that sustainable healthy community is a basic human need, because wherever communities are broken, human beings suffer and well-being declines. This breakdown in Aboriginal communities, has produced a wide range of social problems including abuse, addictions, personal dysfunction, poor physical health, poverty, political powerlessness and collective dependency and despair.
The problems are now well known to everyone. The challenge in community healing is to move beyond the problems to building solutions and even beyond "solutions" (which are problem-generated responses) to rebuilding healthy community life that produces sustainable well-being and prosperity for all.
Relative to
Aboriginal social security reform, community development is the process
of rebuilding the web of relationships (social, economic, political, spiritual,
cultural) so that the common good is again maximized for everyone.
Community Development as a Discipline
The literature in community development as a professional practice and a field of study goes back to the post-war 1950s. As Europe was rebuilding and Africa was de-colonizing, it became increasingly clear that solving critical human problems required the engagement of community members. Top-down, expert-driven approaches were simply unable to effect needed changes of many kinds for challenges such as poverty, community health and ethnic conflict.
In 1954, the British Colonial Office (HMSO) described community development as a "movement designed to promote better living for the whole community with the active participation, and if possible, on the initiative of the community" (HMSO 1954). A decade later, the field was acquiring clearer definitions and methodology. Du Sautoy (1964) explained that community development involved self-help and attention paid to people's felt needs and the social traditions and other aspects of the community as a whole. In Rhodesia, W. Green (1965) borrowed a definition from the U.S. International Cooperation Administration, which called community development "a social process" through which "people became more competent to live and gain control over aspects of a frustrating and challenging world" (cited in Roberts, 1979). This definition shifts the focus from mere self-help to empowerment--the idea that developing people need to discover power within themselves and gain power and some measure of control over the forces that are affecting their lives.
Haydon Roberts (1979:36) defined the process of community development in terms of six interactive phases of activity.
2. Learning (for empowerment) - involves acquiring knowledge of self, ones social reality and one's environment, skills related to communication and group discussion, and attitudes toward self, others and the world.
3. Objectives - involves concrete planning and experimentation.
4. Learning (for action) - involves skills needed to carry out planned actions.
5. Action - refers to deliberate collectively planned initiatives.
6. Evaluation - involves reflection on the effectiveness of the action taken in terms of the community's goals and purposes, and also leading to a deeper analysis of the situation, a clarification of felt needs, and another round of activity (i.e. #1 - 6 above).
In related fields of work, a new approach to adult education which came to be known as "popular education" was emerging, inspired by the work of Brazilian born educator Paulo Freire (1972), Canadian Bud Hall and his colleagues at the University of Toronto, and people like Miles Horton at the Highlander Center in the United States. This lively and engaging approach to educating community people for empowerment and action soon spread around the world and became a primary line of action in community development work. One of the best examples we know of within this genre is the three volume work Training for Transformation: A Handbook for Community Workers (Hope and Timmel, 1984) developed in Zimbabwe, which deal with critical awareness skills for participatory education, social analysis, and community planning, all at a level village people can understand and relate to. Popular education represents a major departure from the academic schooling approach to learning. It places learning in the center of the community development process, and uses a wide variety of learning strategies (mapping, games, theatre, art, simulations etc.) to prepare community people to play their role in community development processes.
Competing Views of Community Development
It is quite possible to listen to five different "experts" and get five different explanations about what community development "really" is, what is important, where to start, what to do or not do, and what success means in community development. We have identified seven distinct approaches within the literature and professional practice of community development. Because community development is so fundamental to Aboriginal community healing and restoration processes, we feel it important to at least briefly comment on the differences between these approaches so that communities can choose pathways most appropriate to their needs.
Seven Approaches to Community Development
The liberation model tends to be blind to basic human relations issues and to the need for personal growth and healing. It also tends to see enemies and conflict but overlooks potential allies and opportunities. As well, it often ignores the spiritual and cultural dimension, and is sometimes blind to the dominant cultural baggage contained within its own models and methods.
The therapeutic model tends to personalize the entire problem of development, such that individual healing is seen as the solution to almost everything. Is often blind to structural inequities embedded in the system, and, in general, seems unable to address the socially constructed nature of the human world. Also, it fails to adequately address the political and economic dimensions, and tends to ignore complex society-level problems such as the environmental crisis, ethnic conflict and poverty, or else to reduce them to the simple problem of the need for healing.
together in a loose coalition.
The issue organizing approach tends to mobilize people around common concerns, but once the issue fades away, the people retreat back into their families and home groups. This approach often blind to the actual challenge of building the human relationships that make up a living community. It tends instead to focus on meetings and getting things done, but is usually operating without an integrative vision of what a healthy and prosperous community would look like and how to get there. It is often dominated by strong personalities who are able to see some issues clearly, but others not at all. It is often unable to grasp the full meaning and importance of people's participation, which tends to be reduced to a means-to-an-end strategy rather than an essential dynamic.
The community organization model tends to gloss over or ignore hard issues (whether interpersonal or structural) and instead to focus on the matters of common concern which are the easiest to resolve (e.g. scheduling of recreation events, spring cleaning the neighbourhood, etc.). It tends to have faith in the system as it is, but believes there is a need for lobbying and advocacy to get what you want. Is not usually concerned with social change or with rectifying basic development problems.
The economic approach is often blind to social concerns of all kinds. It sees such issues as health promotion; education; youth development; or personal, family and social problems as being subsets of the economic development challenge. This approach has historically been so fixated on making money that it is unable to "see" other dimensions of development as having any importance. It tends to be blind to the social determinants of prosperity (such as the relationship of a sobriety movement to productivity), and tends to believe that its own focus on wealth-production makes economic leaders the rightful controllers of society's resources. It tends to be blind to social and economic inequalities that directly influence people's capacity to participate in and benefit from the economic activities of the community.
As important as this approach is, it can be blind to the political and economic dimensions of development, and is sometimes unable to see how to bring the strengths of the past into the process of building a sustainable future. People advocating this approach can sometimes be dogmatic in insisting that its own way of expressing universal truths is the only way. Even in its defence of culture, this approach is sometimes blind to the multicultural nature of the development context, and can be intolerant or blind to the differences in perspective that exist within developing communities (between the younger and older, women and men, more and less educated, powerful and powerless, traditionalist and modernist, etc.).
Because the Ecological Systems model takes an integrative generalist approach, it can seem to be preoccupied with the big picture, leaving real people with very specific problems wondering how they fit in. The model requires a grounded learning process in order to use it, and draws heavily on the knowledge base and skills flowing from many of the other models in order to be effective in the real world. Because of the inclusivity of this approach and the fact that it deals with so many dimensions and aspects, this model can make the solving of critical social and economic problems seem overwhelming and hopelessly complex, and cause some people to retreat into approaches that appear to be easier to use.
Nuts and Bolts
From this summary, it should be clear that it can make a great deal of difference which model of community development influences work in Aboriginal communities. We recommend that for most situations, the ecological system model (which weaves together the principal elements of all the others) is probably the most useful.
When such an integrative and holistic approach is employed, the nuts and bolts of day-to-day work in community development can be described in two broad categories: the inside part and the outside part.
The Inside Part
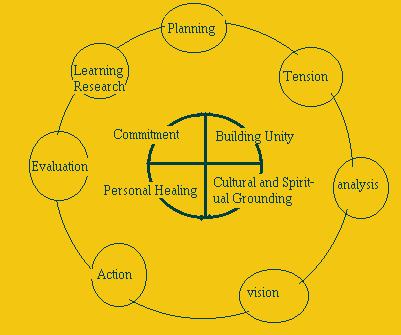
In order for a community to move toward health and well-being, four human development processes need to be going on.
The Outside Part
Here is a brief description of the seven components which can be part of a community development process which is aimed at helping communities address critical social problems. These seven components are presented as a list, but it is important to remember that they do not necessarily happen one after the other in an orderly way. Communities start at different places and will move through the steps in different orders. One step will not be completely finished before another is started, but rather communities can go back to a particular step many times.
Putting it all Together
These four human development processes and these seven components of a community development approach to addressing critical social problems can be pictured in a circle like the one below.
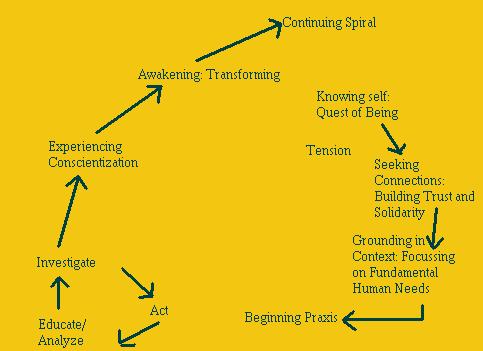
Participation action research (PAR) is a systematic approach to educating, empowering and mobilizing grassroots people for social change which has emerged as one of the most powerful tools yet created for community development. Some of the leading contributors to PAR thinking and practice include Paulo Freire (1974), Bud Hall (1975, 1981), Orlando Fals-Borda and M.A. Rhaman (1991), Rajish Tandon (1981), John Gaventa (1991), William Carr and Steven Kemmies (1986), and more recently, the practice of Arturo Ornelas and Susan Smith (1997).
Participatory action research means engaging grassroots people in a process of investigating their own realities (inner world and outer conditions) with the aim of understanding and transforming that reality. The term "participatory action research" is instructive.
Action refers to the orientation of PAR to transformative movement; i.e. action aimed at producing growth, learning, and improvement in real-world conditions.
Research refers to the work of systematically investigating reality in order to understand how we have co-created it or succumbed to it, are embedded in it, and also what is required in order to change it. Those being researched (i.e. the people, their lives, their community) are also the principal researchers. This is the crux of the PAR methodology.
The process of participatory action research moves through a series of cycles and stages.
Phase One can be called an empowerment phase and it involves:
For several generations in North America (and many other places in the world), people have learned to depend on professionals to fix everything. This has created learned helplessness and dependency thinking in many communities. If there is a social problem, call a social worker. If people are out of work, ask the government to support them or to make jobs for them. Many of us have learned the individualistic mind-set that responds to hearing about community issues by thinking "that's not my problem." The government will take care of it (or the school, or the medical system--someone). We have learned to believe that we are not responsible for one another's well-being. We have given away this responsibility to professionals.
The movement to re-create sustainable life, and to utilize community development as a primary strategy for addressing critical social and economic issues, turns this kind of thinking on its head. Community development thinking argues that the main role of professionals should be to facilitate learning and capacity building of people to address their own problems.
This type of inside-out approach demands that professionals learn an entirely new attitude and skill set than has been taught in most professional training programs to date. The challenge for everyone connected to community development processes is to play out his or her unique role. Professionals must become facilitators, coaches, mentors and technical supporters. Community members need to become designers and implementors as well as benefactors of development initiatives. Organizations at all levels must learn to play their critical role of listening to communities, taking direction from them, adjusting their programming according to that direction, and at the same time providing a kind of "servant leadership" to the process of community development.
This servant leadership requires a delicate balance between two prerequisites. On the one hand, the fledgling community needs a focal centre around which to gather its energy, as well as training and technical support. On the other hand, there is the fundamental requirement that authentic development must be driven from within the community of people the initiative is supposed to benefit (because the main goal of community development is developing people's capacity to create and implement solutions to meet their own social and economic needs). This inside-out (sometimes also called bottom-up) approach is difficult for many professionals to incorporate into their practice, even if they seem able to talk the talk. It is difficult because a) it runs counter to the culture of most helping organizations; b) it seems to contradict the role of the professional as expert provider; and c) it is difficult to incorporate into the timelines and accountability needs of professional agencies. Nevertheless, sustainable community-building often requires professional involvement and help. It is just that it needs that help to occur within the framework of a true partnership in which professionals are really able to take guidance and direction from the community.
G. Leadership
The relationship between leadership and personal, family and community healing has been raised a number of times in the rest of this document and so this section will merely offer a short summary of some of the issues related to this topic.
One of the important aspects of this relationship is the fact that it is reciprocal. Leadership is required in order for community healing to occur but many community leaders require healing themselves in order to become balanced and healthy themselves and to carry out their role effectively.
Community healing requires a network of formal and informal leaders (e.g. elders, front-line workers, elected representatives, traditional leaders, grassroots leaders, etc.) who play the following types of roles. Any individual leader may well play more than one of these roles and each of these roles will likely be carried out by more than one individual.
2. Facilitative Leadership - community leaders who understand the conditions, dynamics and steps of healing work and who know how to create the environment which supports others to make a required commitment and do the necessary work.
3. Strategic Leadership - community leaders who take responsibility for ensuring that a shared vision of community health and well-being is articulated and remains a pivotal focus in all economic and political decisions. These leaders also work toward the transformation of all the community institutions on the basis of life-preserving, life-enhancing values and sound development principles.
4. Healing Leadership - community leaders who can lead healing processes (such as traditional ceremonies and support groups) and/or who can share their knowledge and experience about healing processes with others.
|
|
|
|
| Next-Part IV |